
Tennis & Golfer’s Elbow – A Painful Elbow Tendonitis
Tennis and golfer’s elbow are a frequently occurring problem in today’s active society. Ironically, most patients affected with tennis elbow never played tennis! This condition is characterized by pain over the outside portion of the elbow joint. It is made worse with grasping objects. It can become so severe that it may be difficult to hold on to objects, hold sports racquets write or do other tasks which require grasping an object tightly. This condition has been called “lateral epicondylitis.” The condition was first described by F. Runge in a paper published in 1873.
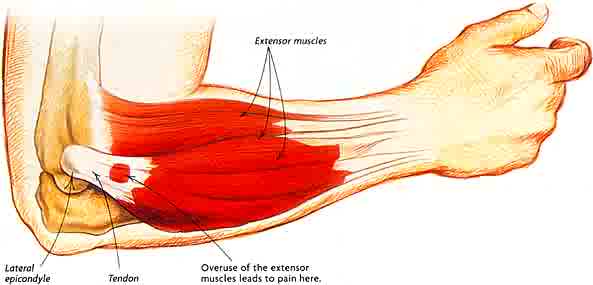
The most characteristic symptom is point tenderness and pain over the outer boney area of the elbow. Grasping objects and wrist extension are what typically make the pain much worse. Tennis elbow can be seen in all ages over 20 but is most commonly seen in individuals between 30-60. There is no gender predominance, nor an increased incidence in individuals who play tennis. The underlying pathophysiology is micro tears that occur in the extensor carpi radialis muscle. This is a small forearm extensor muscle that attaches to the lateral epicondyle of the elbow. Large forces are transmitted through this muscle in activities that involve gripping and wrist extension. Through repetitive extensor motion of the elbow and wrist, this muscle and its associated tendon become traumatized with the resultant micro tears of the tendons. As the tendons connect muscle to bone, it is these tears in the tendon that cause elbow pain, similar to the pain from ankle sprain injuries. Tennis elbow can also be caused by direct trauma to lateral elbow area (author’s personal experience.)
The pain from tennis elbow can vary from mild to extreme. In more severe cases, the pain is present all the time and made worse with most activities that involve grasping and wrist extension. Treatment includes use of anti-inflammatory agents such as aspirin, ibuprofen or naproxen. An elbow brace, with a small pad in it, can be worn. It is important to have the brace properly placed so that the pad lies over the tendon-bone junction and with suffice pressure to aid in the regeneration of tendon fibers to grow onto the epicondyle. Daily exercises to strengthen the extensor carpi radialis should be performed. The easiest way to accomplish this is to use two “fat” rubber bands, similar to the ones used to wrap mail. Put these bands around the fingers (and thumb) of the affected hand. Then spread or fan your fingers out with resistive pressure from the bands. You will see your extensor carpi radialis muscle tighten up. This simple exercise needs to be done literally hundreds of times a day over several weeks to be of benefit. Having treated hundreds of patients over the years, this clearly is the most beneficial treatment, over the long run.
In some cases where the pain is severe, a single cortisone injection can be performed. This relieves the inflammation and pain but must be followed up with splinting and hand exercises. Unfortunately repeated steroid injections can cause tissue breakdown, weakening of the tendon and ultimately more pain. Platelet rich plasma can dramatically benefit patients with tennis elbow. The PRP is injected over the lateral epicondyle and is “peppered” around the area for maximal therapeutic benefit. The PRP is then activated with thrombin, forming a graft over the area. (http://www.orthohealing.com/news/thedoctors-plateletrichplasmatherapydemo-video/ ) This results in dramatic healing and regeneration of the extensor carpi radialis tendon and growth back onto the lateral epicondyle. Pain relief usually occurs within 2-3 weeks of the injection. The final outcome is a stronger tendon and dramatic improvement in quality of life. If you have elbow pain, ask your doctor if you may be a candidate for PRP therapy.